Cuboid Foot
, and 'Oh my God, just END!!!' I know I'm the minority preferring Drakkhen to Dragon View, but hey, different strokes for different folks.That ending was painful for me it wasn't funny (and actually affected the entire quality); there were moments watching it when I was like 'Go on!' , 'Get to the point already!' I'm one of those people who will stick through an entire game (and movie) no matter how good or bad (credits and post-credits sequences included), and with Dragon View I just. Dragon view snes rom download.
Did you know that there are some similarities between athletes and ballet dancers? One of the easiest comparisons between athletes and ballet dancers are the injuries. Both groups can be afflicted with particular injuries that you don’t usually get without doing a sport or performing ballet.
Manipulation of the cuboid is perhaps one of the easiest yet most rewarding of all foot mobilizations. Several types of techniques exist, but the aim of this article is to describe the simplest and most gentle method. The key to a successful yet gentle procedure involves accurate diagnosis of a cuboid. Best shoes for cuboid syndrome helps to keep your foot and ankle from all the pain generated from cuboid bone ligaments and joints injury. Suffering from cuboid syndrome exposes you to severe pain on your lateral foot side which is also the side of your little toe get yourself thecorrect footwear 100% keeps your foot from Cuboid syndrome foot pain.
Take cuboid syndrome for instance.Cuboid syndrome is a type of injury that affects a particular bone in the foot, and it appears quite commonly in athletes and ballet dancers. But why is it so common between those two? What are cuboid syndrome symptoms?
What are cuboid syndrome treatments? We’ll cover all of this and more, so if you’re curious, keep reading. The Causes and Symptoms of Cuboid SyndromeThe first thing you need to know is what cuboid syndrome is. Cuboid syndrome is when the cuboid (one of the five bones that make up the midfoot) becomes partially dislocated due to repetitive injury, ankle sprain, or severe trauma.
These are the types of injuries associated with ballet dancers, runners, and any sport that features similar movements.The cuboid is a bone that is key to stabilization of the outer midfoot and helps distribute your body’s weight. When you have cuboid syndrome, there are several symptoms that can affect your day to day life.These symptoms include the following:. Difficulties in walking. Acute or chronic aching pain on the outer side of the foot.
Lateral part of the foot is tender to the touch, and is red and swollen. Pain increases when the patient walks or puts pressure on the foot. Pain usually reduces after complete restThe midfoot is uncomfortable or painful. The patient may have issues with pain if they are hopping on one foot, assuming they can even hop on one foot, or will more than likely walk funny.
They may also experience a decrease in motion, and ankle movements can be painful, especially inversion.As you can see, unless you are a doctor, some of the symptoms could be related to different types of foot injuries. So, how do you know that you have cuboid syndrome? Diagnosis of Cuboid SyndromeCuboid syndrome is rather hard to diagnose. The symptoms that we previously mentioned are very similar to many symptoms of other foot injuries. It’s due to this that a regular doctor may refer you to a podiatrist, a doctor that specializes in the foot and foot injuries.The podiatrist will ask you about your physical activities and past injuries to the foot and ankle area.
While imaging tests like x-rays may be used, cuboid syndrome will usually be diagnosed through physical tests and exams. Midtarsal Adduction TestStabilizing the ankle joint with the right hand, the podiatrist will take their left hand and hold the foot around the midpoint and move it inward towards the other foot. Doing this compresses the patient’s calcaneocuboid joint and may cause the symptoms of cuboid syndrome. Midtarsal Supination TestThe podiatrist stabilizes the ankle joint while he or she manipulates the foot in roughly a half-circle. This motion will also cause the pain of cuboid syndrome.After these tests, if the diagnosis comes back as cuboid syndrome, you can then begin treatment. Treating Cuboid SyndromeNow that you have a diagnosis of cuboid syndrome, you can move on to treat it.
Your podiatrist will recommend one or two courses of action to help you get back on your feet. RelocationThe first step and possibly the most painful is relocation. This procedure should only be performed by a medical professional, as it involves the cuboid bone being moved back into place.
It is done in a thrust motion and may hurt. After relocation, you can move to the next steps to heal the area that the dislocation may have injured.
RestRest can help most strains and pulls. It can give the tissue around the cuboid bone time to heal. You’ll be told to stay off the afflicted foot as much as possible for a certain amount of time. You may have to use a wheelchair and crutches to help keep the weight off your foot so that you can still do things. ImmobilizationThe podiatrist will tape, pad, and use compression bandages to immobilize your ankle and foot so everything can heal into place.
The padding can help minimize reinjury. Cold CompressA cold compress or ice pack can help reduce swelling and pain on your injured foot. The ice pack should be applied for 5 to 6 minutes at a time, three times a day. OrthoticsOrthotics are prescription foot appliances that can help everything stay in place on your foot. ExercisesAfter the foot has healed a bit, you will need to perform certain foot exercises to build up strength and flexibility.Hopefully, with these treatments, your foot will be as good as new. Cuboid Syndrome Takes Time to HealCuboid syndrome hurts, and it can be uncomfortable. It can make walking and moving a pain, but luckily, it’s very treatable.
The most important thing to remember is not to rush the healing time.More than anything else, cuboid syndrome takes time and patience to repair. If you rush through your treatment, you may cause future injury. If you take your time and follow the doctor’s orders, you may be able to come back as good as new.Sources:“Cuboid Syndrome – Causes, Symptoms, Treatment & Exercises,” Pain Care;.Armstrong, K., “Cuboid Syndrome: Symptoms and Treatment Options,” Foot Vitals, October 30, 2015;.“Cuboid Syndrome,” Foot Pain Explored;. Disclaimer: The information contained herein is for information purposes only and is not to be construed as a diagnosis, treatment, preventive, or cure for any disease, disorder, or abnormal physical state, nor should it be considered a substitute for medical care from your doctor. On any matter relating to your health or well-being—and prior to undertaking any health-related activity—consult an appropriate health professional.
The opinions herein are exactly that, they are the opinions of the author. Doctors Health Press and its employees are not responsible for medically unsupervised activities that could be harmful to your health.
Results are not guaranteed. and may vary from person to person. All of the Doctors Health Press publications come with a 100% satisfaction guarantee. If you’re not satisfied with your newsletter, you can simply cancel your subscription and receive a pro-rated refund on all undelivered issues.
For our books and special reports, we will give you a full refund of your purchase price within 30 days of your order. We pride ourselves on excellent customer service. Disclaimer: The information contained herein is for information purposes only and is not to be construed as a diagnosis, treatment, preventive, or cure for any disease, disorder, or abnormal physical state, nor should it be considered a substitute for medical care from your doctor. On any matter relating to your health or well-being—and prior to undertaking any health-related activity—consult an appropriate health professional. The opinions herein are exactly that, they are the opinions of the author. Doctors Health Press and its employees are not responsible for medically unsupervised activities that could be harmful to your health. Results are not guaranteed.
Shoppe keep game free download. and may vary from person to person. All of the Doctors Health Press publications come with a 100% satisfaction guarantee. If you’re not satisfied with your newsletter, you can simply cancel your subscription and receive a pro-rated refund on all undelivered issues. For our books and special reports, we will give you a full refund of your purchase price within 30 days of your order.
We pride ourselves on excellent customer service.
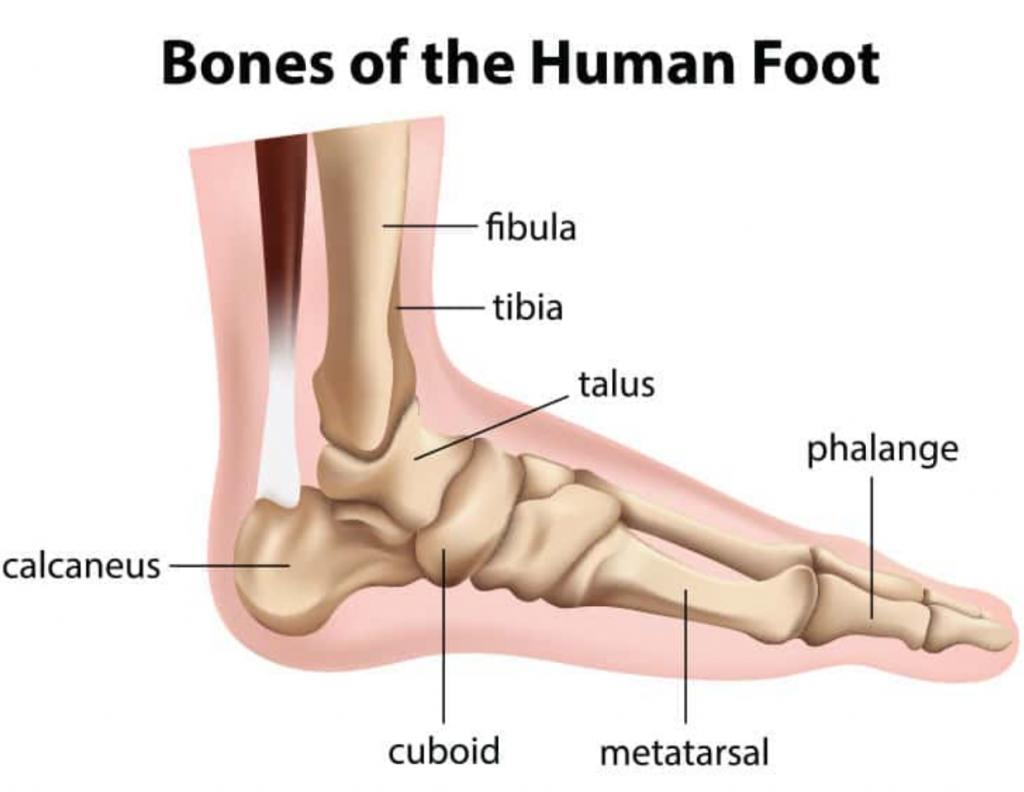
Bones and Joints of the Foot and Ankle OverviewFigure 1: Bones of the Foot and AnkleRegions of the foot: Figure 2: Regions of the Foot. Hind-foot – as the name suggests, the hindfoot is the portion of the foot closest to the center of the body.
It begins at the ankle joint and stops at the calcaneal-cuboid joint. Mid-foot – The midfoot begins with the calcaneal-cuboid joint, and essentially ends where the metatarsals begin. While it has several more joints than the hind-foot, it still possesses little mobility. Fore-foot – the fore-foot is composed of the metatarsals and phalanges. The bones that comprise the fore-foot are those that are last to leave the ground during walking.Mobile Joints of the foot and ankle:(See Figure 3.). Ankle joint. Sub-talar joint.
Talo-navicular joint. Metatarso-phalangeal (MTP) joints.Joints that move a moderate amount:. Calcaneal-cuboid joint. Cuboid-metatarsal joint for the fourth and fifth metatarsal. Navicular-cuneiform joints. Joints of midfoot or “Lisfranc” Joint (a.k.a. Tarso-metatarsal (TMT) joints or cuneiform-metatarsal joints)Figure 3: Common Joints of the Foot and AnkleBones of the lower leg and hind-foot: Tibia, Fibula, Talus, Calcaneous.
Tibia and Fibula (Long Bones)Though the tibia (commonly called the shin bone) is not a part of the foot, it plays an important role. The foot is connected to the body where the bones of the foot and ankle meet the tibia and fibula (the small bone to the outside of the tibia). The tibia is also responsible for holding up 85% of the weight that presses down on the foot in the standing position.
The tibia and fibula are held together by a tough layer of connective tissue, known as the Interosseous Membrane. The membrane thickens at the lower part of the leg, in order to make the ankle more stable. These two bones connect with the talus by forming a sort of dish which the talus fits into.
This dish is known as the mortise of the ankle joint. TalusThe talus is something of an odd bone because of its strange shape and the fact that 70% of this bone is covered with hyaline cartilage (joint cartilage). The talus acts as a “ball joint”, playing the critical roll of connecting the lower leg to the foot. The talus is covered by so much cartilage because it connects so many different bones. The talus holds the ankle together by connecting to the lower leg with a ball joint, connecting to the calcaneous on the underside through the subtalar joint, and by helping connect the back part of the foot (hindfoot) to the midfoot via the talo-navicular joint. These series of connections allow the foot to rotate smoothly around the talus, as when you roll your ankle in a circle. Unfortunately, the talus has relatively poor blood supply, which means that injuries to this bone take greater time to heal than might be the case with other bones.
Parts of the TalusThe talus is generally thought of as having three or four parts (Figure 4):. The talar body including the “dome” of the talus. The talar neck.
The talar headThe talar body is roughly square in shape and is topped by the dome. It connects the talus to the lower leg at the ankle joint. The talar head interacts with the navicular bone to form the talo-navicular joint. The talar neck is located between the body and head of the talus, and is remarkable because it is one of the few areas of the talus not covered with cartilage, and is one of the few places that blood can flow to in the talus. Figure 4: Talus AnatomyCalcaneus (The Heel Bone)The calcaneus (Figure 5) is commonly referred to as the heel bone. The calcaneus is the largest bone in the foot, and along with the talus, it makes up the area of the foot known as the hind-foot.
The calcaneus is something like an oddly shaped egg; hard cortical bone on the outside covers softer cancellous bone on the inside. There are three protrusions on the top surface of the calcaneus (the posterior, middle, and anterior “facets”) that allow the talus to sit on top of the calcaneus, forming the sub-talar joint.
The calcaneus also joins to another bone at the furthest end, away from the lower leg and toward the toes. At this end, the calcaneus connects to the cuboid bone to form the calcaneal-cuboid joint. Figure 5: Calcaneal AnatomySubtalar JointThe talus rests above the calcaneous to form the subtalar joint. However, the talus does not sit directly on top of the calcaneus. Instead, it rests slightly offset toward the outside of the foot (the side nearest the little toe). This positioning allows the foot to cope with uneven terrain because it allows a little more flexibility from side to side. The subtalar joint doesn’t move independently; it moves along with the talo-navicular joint and the calcaneo-cuboid joint, two joints located near the front of the talus.
Bones of the Mid-foot: Cuboid, Navicular, Cuneiform (3) Figure 6: Bones of the MidfootCuboidThe cuboid bone is the main bone of the mid-foot. It is a square-shaped bone on the outside of the foot, and possesses several places to connect with other bones.
The main joint formed with the cuboid is the calcaneo-cuboid joint. Farther along its length, the cuboid also connects with the base of the fourth and fifth metatarsals (the metatarsals of the last two toes).
On the inner side, it also connects with one of the lateral cuneiform bones. Calcaneo-cuboid JointThe calcaneal-cuboid joint attaches the heel bone to the cuboid. NavicularThe navicular is located in front of the talus and connects with it through the talo-navicular joint. The navicular is curved on the surface nearest the ankle. The side farthest from the ankle joint connects to each of the three cuneiform bones. Like the talus, the navicular has a poor blood supply. On the inner side (closest to the middle of the foot), there is a piece of bone that juts out, which is called the navicular tuberosity.
This is the site where the posterior tibial tendon anchors into the bone. Talonavicular JointAs the name suggests, the talo-navicular joint connects the talus to the navicular. The curve of the navicular is designed to connect smoothly with the front surface of the talus. This joint allows for the potential to have significant motion between the hindfoot and the midfoot, depending on the position the hindfoot is in. CuneiformsThere are three different cuneiform bones present side-by-side in the midfoot. The one located on the inside of the midfoot is called the medial cuneiform. The middle cuneiform is located centrally in the midfoot, and to the outside is the lateral cuneiform.
All three cuneiforms line up in a row and articulate with the navicular, forming the naviculo-cuneiform joint. The structure of the cuneiforms is similar to a roman arch. Each cuneiform connects to the others in order to form a more stable unit. These bones, along with the strong plantar and dorsal ligaments that connect to them, provide a good deal of stability for the midfoot. Bones of the Fore-foot: Metatarsals (5), Phalanges (14), Sesmoid Bones (2) MetatarsalsEach foot contains five metatarsals. These are the long bones that lead to the base of each toe.
The metatarsals are numbered 1-5, starting on the inside and leading outward (from big toe to smallest). Each metatarsal is a long bone that joins with the mid-foot at its base, a joint called the tarsal-metatarsal joint, or Lisfranc joint. In general, the first three metatarsals are more rigidly held in place than the last two, although in some individuals there is increased motion associated with the 1st metatarsal where it joins the midfoot (at the 1st tarso-metatarsal joint), and this increased motion may predispose them to develop a bunion.The long part of the metatarsal bone is known as the metatarsal “shaft”, and the thick end of the bone nearest the toes is known as the metatarsal “head” (the metatarsal neck lies between the shaft and head). The head serves two very important functions:. First, the metatarsal heads are the locations where weightbearing takes place. Second, the phalanges connect to the foot at the metatarsal heads at a joint called the metatarsal-phalangeal joint.
These joints are very flexible, allowing the metatarsal heads to continuously support the weight of the body, as the foot moves from heel to toe.First Metatarsal – The largest of the metatarsal, both in terms of length and width.Second Metatarsal – The fore-foot is made extremely stable not only by the ligaments connecting the bones, but also because the second metatarsal is recessed into the medial cuneiform, in comparison to the others. The second metatarsal may be overly long in some individuals, predisposing them to 2nd.Fourth and Fifth Metatarsal – The fourth and fifth metatarsal may have greater range of motion than the others do. PhalangesThe phalanges make up the bones of the toes. They are connected to the rest of the foot by the metatarsal-phalangeal joint. The first toe, also known as the great toe due to its relatively large size, is the only one to be comprised of only two phalanges.
These are known as the proximal phalanx (closest to the ankle) and the distal phalanx (farthest from the ankle).The four “lesser toes” (toes 2-5) all have three phalanges. The phalanx closest to the ankle is known as the proximal phalanx, which articulates with the “middle” phalanx, the proximal interphalangeal joint (PIP joint). The middle phalanx meets the “distal” phalanx at the distal interphalangeal joint. An imbalance in the tendons pulling across these small joints of the toes will lead to deformity of the toe, such as a. A list of the joints of the toes can be found below (Figure 7).

Inter-Phalangeal Joint (great toe only). Proximal Inter-Phalangeal Joint (PIP joint – toes 2-5). Distal Inter-Phalangeal Joint (DIP joint -toes 2-5)Figure 7: Joints of the ToesSesamoid BonesA sesamoid bone is a bone that is also part of a tendon. An easy example of such a bone is the kneecap (patella). In the foot, there are two sesamoid bones, each of which is located directly underneath the first metatarsal head. These seasmoids are part of the flexor hallucis brevis tendon.Edited October 17, 2015mf/ 7.31.18.